Fructose gets hammered by the blogosphere as an evil sweetener. It has been blamed as a major cause of obesity, diabetes, and inflammation related diseases. The hyperbole surrounding it can get nauseating at times, especially when there is an obscene amount of literature.
Part of my job as an educator is to try and shed light on big topics and get to the truth in a way that brings the learner (in this case the reader) along on the journey.
Instead of just stating something like, “fructose is fine”, I would rather walk through the evidence and show you my thought process and conclusions and then you can decide whether you accept or reject my conclusion.
This NutriWiki goes a little deeper and a tad nerdier than normal, but it is important that we get into the weeds with this one.
You have to understand the facts about fructose metabolism in humans and why dosing and study design really, really matter when drawing conclusions. With those ideas percolating in your cortex we can begin.
The Epidemiological Evidence
The idea that fructose, especially high fructose corn-syrup, is “evil” and obesegenic arises from a lot of epidemiological data and animal data.
For example, several papers have shown an association with fructose/high fructose corn syrup intake with BMI, obesity, and type 2 diabetes (1, 2, 3). Now there are several things to consider here before we jump to the “that suggests fructose is bad” conclusion.
I want to start with the simplest aspect. Epidemiology data generates hypotheses, it does not even come close to causation or even imply a direct link. This is most easily demonstrated by the ice cream and shark attacks example.
It goes like this, “A study was just published showing that ice cream consumption was highly associated with shark attacks, this suggests that consuming ice cream may cause shark attacks”. Now that seems pretty unlikely.
The real story is probably that people consume more ice cream during the summer, during which they are also spending more time swimming in shark infested waters.
There is also the contradicting literature wherein fructose and HFCS intake doesn’t really show strong associations (4, 5). While the contradicting literature doesn’t negate the early findings it does suggest a more complicated picture.
With that segue way, we can move onto the more complicated aspect of those epidemiological findings, the behavioral and the biological.
The Behavioral Component
The behavioral aspects and the “higher order” effects really need to be considered when interpreting the epidemiological data.
When looking at these papers the authors often “control” for things like smoking, body weight, caloric intake, exercise etc. We often make the false assumption that controlling for those variables statistically means we have isolated the role of fructose, this is far from reality.
For example, someone who consumes large amounts of HFCS (i.e. drinking 2 liters of mountain dew a day) is also more likely to engage in other “non-healthy” lifestyle behaviors like smoking, being sedentary, over consuming calories, eating other potentially foods detrimental to our health.
This type of scenario, which is more the norm than the exception, cannot be truly captured by controlling for covariates mathematically, it just doesn’t work that way.
In my view, the epidemiological data is interesting, hypotheses generates, and provides the foundation for systematic inquiry to elucidate the biological aspect.
Fortunately there has been several systematic inquiries into the role of fructose in obesity, inflammation, and diabetes. The story that unfolds in the literature is fascinating and worth diving into feet first.
The Biological Data
The biological is where things actually get interesting and fun. We get to sort out the hard data. But before we get into the weeds of the science I want to give you a brief primer on fructose metabolism and clear up some of the confusion surrounding it.
I want to break it down clearly and succinctly (you all didn’t come here to read convoluted biochemistry). This is also incredibly important to the main question at hand: is fructose per se really a bad thing for you?
First of all, we have to turn to human studies as mouse metabolism doesn’t always translate well to humans. We have a plethora of human data available so I think we should rely on that data and not the mouse data.
Let’s review what happens in humans when we consume fructose (for a more robust look at these data please see citation 6.
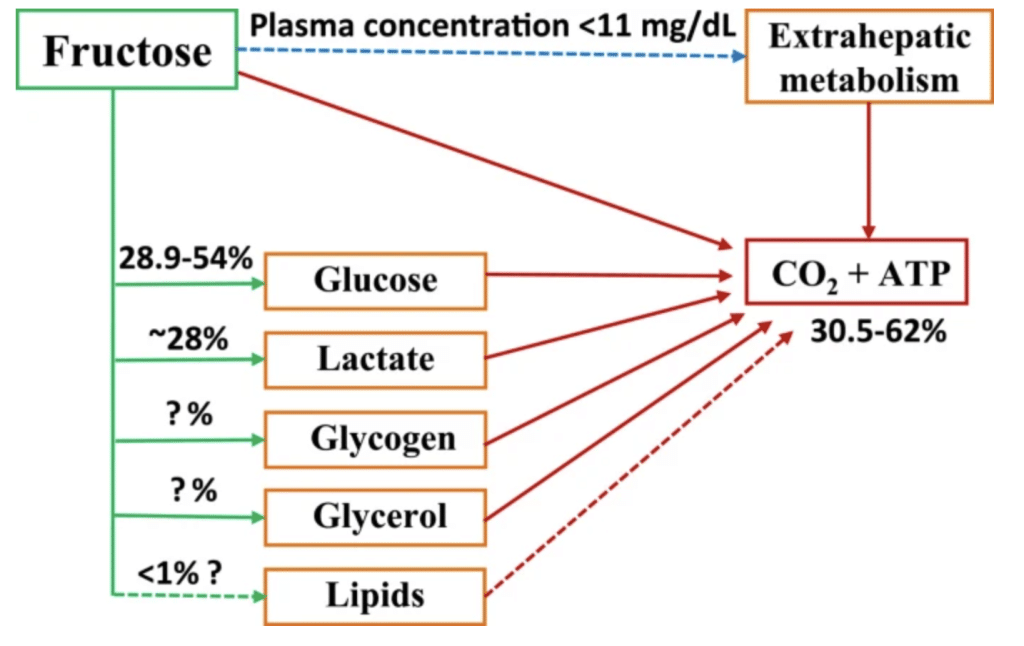
- When consumed, a large portion of fructose is oxidized fairly quickly by the liver (data shows anywhere from 38% to 82% is oxidized within 6 hours) (6). This has been validated by isotopic tracer studies.
- When consumed, a decent portion of the fructose is converted to glucose by hexokinase and phosphoglucose isomerase (The data shows anwhere from 22% to 56% of fructose is converted to glucose within 6 hours of consumption)(6). This has been validated by isotopic tracer studies.
- When consumed, some of the fructose is converted to lactate and exported from the liver into the blood stream. Several studies have shown this but I really like this figure from a paper by my friend Jorn Tromellen that shows this effect in the context of fructose as a peri workout sugar. This also has been validated by isotopic tracer studies but the direct quantification of percentage is more difficult due to the nature of metabolism of fructose to lactate
- Now for the most controversial one. When consumed, some fructose is indeed converted into VLDL triglycerides. By nature, this metabolic process presents limitations in methodology so only two studies have been done with isotopic tracers that allow us to get a good picture of what is going on. In one study, the authors showed that lipogenic potential of fructose seems to be small, since only 0.05% and 0.15% of fructose were converted to de novo fatty acids and TG-glycerol at 4 hour, respectively (7). Fructose actually appears to alter current lipid metabolism by favoring esterfication but does not itself contribute to fatty acid synthesis to any meaningful extent. I.e. the conversion of fructose to any lipid is almost meaningless at normal to slightly high intakes (0.75 g/kg)
- Here is what the overall breakdown of fructose metabolism looks like based on what we have learned from isotopic tracer studies.
- Co-consumption of modest amounts other carbohydrates along with fructose appears to alter fructose metabolism but only slightly. However, the fraction of fructose that gets converted into VLDL TG is likely to increase when consumed in large quantities by itself (AKA 2 liter of Mountain Dew), or in co-consumption with another meal (1 liter of Mountain Dew and a large pizza). If you are concerned about your health, don’t do either of those very often.
I think that sets the stage fairly well and allows us to have context going into the actual studies done on humans and how I arrived at the last point
The Dosing Problem
One of the most important aspects of reading and interpreting scientific literature is context. This is exceptionally true when we dive into the fructose literature.
When you look at the literature that has caused the sensationalised articles like, “fruit makes you fat”, they often fail to notice the major issues with the studies; the dosing problem. One of the things we see consistently in the literature is that extremely high intakes of fructose result in poor health outcomes.
For example, feeding healthy young males (n=55) either 3 grams of glucose or 3 or 4 grams of fructose per kg of body weight for 6-7 days decreased insulin sensitivity and increased fat content in their liver. In the exact same study, consuming 1.5 grams of fructose per kg of body weight per day did not effect insulin senstivity or fat content in their liver.
Now this is interesting. Essentially this data suggests that if you were to feed me (85kg male) 255 grams of straight glucose, 255 grams of straight fructose, or 340 grams of straight fructose per day and not really exercise that I would see decreases in insulin sensitivity and have some liver fat accumulation, but it would not occur if you fed me 127.5 grams of fructose. Keep this data in your mind to refer to in our discussion below (8).
In a different study, obese men (n=9) and women (n=8) consumed 30% of their total daily calories from either glucose or fructose sweetened beverages and the authors measured their hormonal and biochemical response to the feeding over a 24 hour window.
Now I did some digging and was able to figure out the diets they were given. The mean food intake was around 1800 calories which means that each person received, on average 135 grams of glucose or fructose.
The authors didn’t provide body weight so we can’t extrapolate to g/kg doses but lets just say 135 grams of glucose or fructose from sugar sweetened beverages is a substantial amount, like 6 cans of coke a day.
In this study, fructose led to greater post prandial serum levels of lactate and fructose but surprisingly had lower levels of plasma free fatty acids than glucose. Interestingly, the serum triglycerides were higher, suggesting that the TG exportation mechanisms were upregulated in the liver (9)
Now there is some nuance to this triglyceride data when they broke it down into insulin sensitive and insulin resistant individuals.
When you look at the data it appears that being insulin resistant “eats up” most of the variance seen by the increase in triglycerides and once that is accounted for that there is a small difference between postprandial serum triglycerides with fructose being a bit higher.
So our conclusion from this study is, if you consume 130 grams of sugar sweetened beverages containing either glucose or fructose you see increases in serum triglycerides. Fructose appears to lead to slightly higher levels of triglycerides but lower free fatty acids.
If you are insulin resistant your triglycerides will be much higher, regardless of fructose or glucose. To optimize postprandial serum lipid measures don’t consume unnecessarily large quantities of fructose or glucose every day.
These are just two examples of many showing that substantially high amounts of fructose can modulate triglycerides and alter hormonal signaling that favor a “metabolically unhealthy” environment.
But these artificial scenarios don’t really represent what we see in free living situations. Yes, some people may consume unfathomable amounts of fructose, but for the large majority of us the real question ought to be, what do normal intakes of fructose do? Well I am glad you asked, we can explore that research too.
In order to discuss the role of “normal” intakes of fructose we need to review the consumption data. Based on NHANES survey data (not 100% accurate but it gets us close), the mean consumption of fructose was estimated to be 54.7 g/day (range, 38.4–72.8) and accounted for 10.2% of total caloric intake.
Consumption was highest among adolescents (12–18 years) at 72.8 g/day (12.1% of total calories). One fourth of adolescents consumed at least 15% of calories from fructose. The largest source of fructose was sugar-sweetened beverages (30%) followed by grains (22%) and fruit or fruit juice (19%) (10).
So clearly the studies above are substantially missing the mark in terms of dosing. Thus, as so eloquently put by Geoffry Livesy in his review, “By focusing on the adverse effects of very high and excessive doses, we risk not noticing the potential benefits of moderate to higher doses, which might moderate the advent and progress of type-2 diabetes, cardiovascular disease, and might even contribute to longevity.
A salutary rather than hyperbolic examination of the evidence base needs to be undertaken”. I couldn’t agree more.
In a meta-analysis and meta-regression Livesy conducted on fructose intervention trials he began to tease out the “dose response question” (11). In their analysis they found that when pooling 14 randomized control trials that included a combination of all health types, fructose intakes up to 100 grams per day had no effect on fasting plasma TG.
This effect remained even if they swapped out fructose for starch, glucose, or sucrose. Importantly, their analysis showed that plasma TG did increase inline with the previous studies when they did a random effects regression looking at intakes over 350 grams per day, demonstrating their analysis matched the actual data from the studies.
When they then applied their analysis to the normal levels of intake, as noted above from the NHANES data, they were able to show that fructose intake <100g/day did not have an impact on body weight.
Together, this data suggests that it is not the fructose per se but the overall energy intake that drives much of the observed epidemiological data. This brings us back to the point of statistical controlling of covariates not being a robust control in many circumstances.
I don’t want to just take Livesy’s “word” or analysis as gospel, rather I want to dive a bit deeper and explore a few more pieces of literature on this topic.
A very thorough review of the literature titled, “Evidence-Based Review on the Effect of Normal Dietary Consumption of Fructose on Development of Hyperlipidemia and Obesity in Healthy, Normal Weight Individuals” was conducted by Dolan et al. and published in 2009 in Critical Reviews in Food Science and Nutrition (12).
The review was incredibly extensive, exhaustive (at the time) and screened studies quite critically. A detailed report of their review is beyond the scope of this article but a few highlights will get the main points across quite nicely (See original review for studies cited below).
- In a high quality seven day, randomized, crossover study conducted by Sunehag et al. (2002), twelve healthy, non-obese adolescents (six males, six females) were maintained at home on prepared, isocaloric diets containing 60% carbohydrate, 25% fat, and 15% protein, with 10% or 40% of the carbohydrate (6 or 24% of dietary energy) content provided by fructose (low fructose or high fructose diet, respectively). . . The total amounts of fructose ingested in the low and high fructose diets were estimated to be 36 and 133 g/day in females and 40 and 136 g/day in males. A different group of twelve subjects also was exposed to a high carbohydrate/low fat diet or a low carbohydrate, high fat diet, with 20% of carbohydrate as fructose (approximately 55 g/day fructose). Therefore, the ability of fructose to affect biochemical parameters (e.g TG, glucose, insulin, the insulin by product C-peptide, or free fatty acid) in a dose-dependent manner could be assessed. In this study, the increase in dietary fructose had no effect on any of the parameters that were measured, indicating that fructose has no effect on lipid or carbohydrate metabolism when the caloric intake of individuals is not increased. (ref)
- In a moderate quality, randomized, crossover study, the effect of ingestion of an energy balanced (control) diet or a diet with a 50% excess energy (approximately 914 kcal/day) provided as fat (approximately 57.1 g/day), or glucose, fructose, or sucrose (approximately 123 g/day) for four days on energy balance was assessed in eight normal weight and five obese women (McDevitt et al., 2000). The study was conducted in-house, in a whole body calorimeter. There were no significant differences between normal weight and obese women in macronutrient oxidation or balances, so data were pooled. Over-consumption of glucose, fructose, or sucrose induced glycogen storage on Day 1 (approximately 100 g), but thereafter stimulated carbohydrate oxidation so that balance was achieved on Days 3 and 4. Fat oxidation was proportionally suppressed by sugar ingestion. There were also no significant differences between the various sugars in carbohydrate oxidation, carbohydrate balance, energy balance, fat oxidation, or fat balance. On average, 12% of the excess energy was stored as glycogen and 88% as fat for all dietary conditions (including overconsumption of fat). This study shows that ingestion of a high fructose diet did not disproportionally stimulate fat storage compared to glucose or sucrose and that the net effect of overconsumption of sugar on fat balance (regardless of type) is similar to an excess of dietary fat. (ref)
- Bantle et al. (2000) conducted a crossover study (score = 32) in 24 healthy subjects (12 per sex) ingesting prepared, isoenergetic diets (55% carbohydrate, 15% protein and 30% fat) over a course of 42 days. Diets were nearly identical in nutrient composition, with the exception that 17% energy (341 kcal) came from crystalline fructose in one diet and 14% crystalline glucose (280 kcal) plus 3% crystalline fructose (60 kcal) in another diet. The amount of fructose in 2000 kcal diets was approximately 80 g (high fructose diet) and 10 g (low fructose diet). . . .Throughout the study, fasting or postprandial plasma TG of women was not affected by consumption of either diet. Men ingesting the high fructose diet had significantly greater fasting and postprandial TG concentrations than men ingesting the low fructose diet throughout the study. However, over the course of the study, fasting plasma TG decreased in both groups (with respect to baseline). The fructose diet had no significant effect on fasting plasma cholesterol, HDL-C or LDL-C in either men or women (values for these parameters decreased over the course of the study regardless of diet). At the end of the study, the body weights of the subjects ingesting the high fructose or low fructose diets were not significantly different from each other. Over the course of the study, both groups lost approximately 1.3 kg, indicating that if caloric intake is controlled, the consumption of a high fructose diet can actually result in weight loss.
When you review the studies presented in this paper you begin to put some pieces together and a fairly clear picture emerges.
Based on the current data, there is no real evidence demonstrating that ingestion of up to approximately 100 g/day fructose instead of glucose or sucrose is associated with an increase in food intake or body weight and that despite relatively high levels of fructose you can lose body weight in a hypocaloric state.
So it appears that moderate amounts of fructose don’t alter the metabolic milieu enough to make it “obsegenic” per se. Additionally, in both healthy and obese subjects, moderate intakes of fructose don’t appear to result in changes in fasting serum TG.
Much Ado About Nothing?
Right now you probably feel like you just drank from a fire hose of biochemistry, clinical trials, and my attempt at science communication. Let me take everything we have learned over the course of this article and distill it down into a single thought.
Fructose consumption at moderate levels of intake do not adversely effect body weight or blood chemistry based on the current data. Obscenely high levels of intake (>150 grams per day) may have undesirable health effects.
Together, these two concepts essentially tell us: 1) that we can consume 3-4 servings of fruit a day, if we so desire, with no health consequences, and 2) that we should not mainline 2 liters of Mountain Dew or consume large amounts of fructose or HFCS.
Conclusion
Now we need to frame this entire thing in the most correct and objective light we can, so let me offer a few more thoughts to close. Clearly the consumption of large amounts of fructose through HFCS is not ideal.
I don’t want to sweep the problem of the increasing sugar (including HFCS) intake under the rug, it is a problem; although data suggests that sugar consumption may actually be declined. It is also important to examine the increase in HFCS and fructose intake from the increasing energy intake standpoint; the added HFCS appearing in our diet isn’t displacing other foods or sources of energy in most situations, rather it is additive.
The current food environment makes it feasible to consume large amounts on any given day. It is even easier if your food choices are “pretty poor”. We should, in my opinion, begin working with industry to start reducing the added HFCS to food, along with other ingredients, to reduce the energy density and palatability of our packaged foods.
But we also need to be honest and sane about our behaviors. We do not need to put on our tinfoil hats; all the pomp and circumstance about apples and bananas being potentially problematic because of 10 or so grams of fructose is likely unwarranted.