Tl;dr: It appears that basal fat metabolism is the most “disturbed” aspect of metabolism in diabetes.
The title of this piece alone should be enough to make you scratch your head. I mean everyone and their dog knows people with a “messed up” metabolism or type 2 diabetes (T2DM) has a carbohydrate/sugar problem right? Well, it turns out it may be the exact opposite. At a fundamental level, individuals with T2DM actually have a fat metabolism problem, not a carbohydrate problem as previously believed.
Now how can this be? I mean blood sugar is elevated in these individuals and they also have “insulin resistance” so clearly it has to be a carbohydrate metabolism problem. Right?! Well let us ask ourselves a basic question that should ferret that out.
What would the baseline metabolism of a person with diabetes be if the underlying cause was in fact, impaired carbohydrate metabolism?
If true, they would have a lower carbohydrate metabolism to fat metabolism ratio than a lean, healthy person. Thus, their respiratory exchange ratio (carbs-to-fat oxidation ratio aka RER) should be lower.
Here is a brief synopsis of RER.
This figure below should give you some idea of what RER looks like in application.
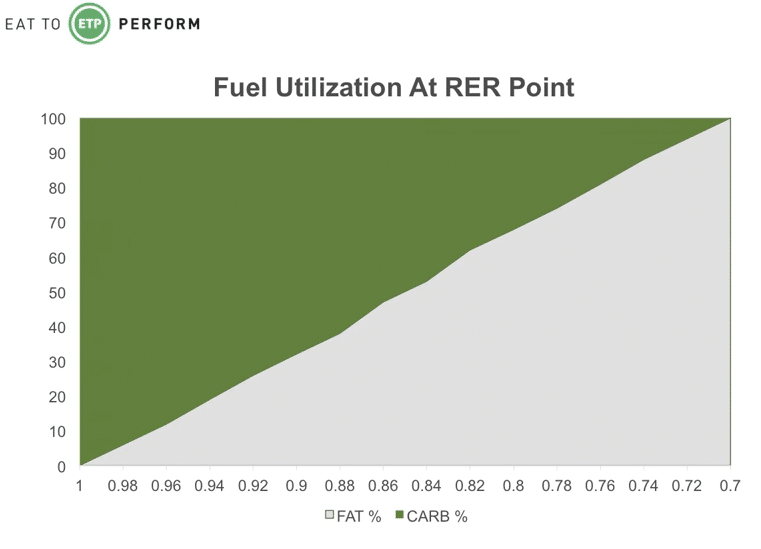
Essentially, an RER of 1.0 means you are burning virtually 100% carbohydrates and an RER of 0.7 means you are burning virtually 100% fat.
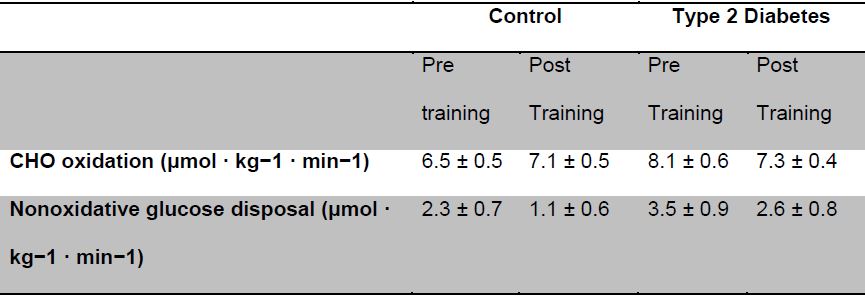
Now that we have an understanding of RER, we can tackle question # 1. When you look at the data we actually see that individuals who have “impaired metabolism” actually have a higher carb-to-fat oxidation ratio, meaning they actually are burning more carbs at baseline (1,2). Importantly, it appears that much of the “extra” carbohydrate utilization occurs in nonoxidative metabolism; meaning it never goes through the mitochondrial and the electron transport chain (Table 1).
Importantly, this hints at a reduced mitochondrial function and also likely some issues with the beta-oxidation of fat (a separate process from the primary mechanism of creating energy from fat). Think of it like prepping the ingredients for a meal. . . it is a necessary step, but you still gotta cook the ingredients afterwards!
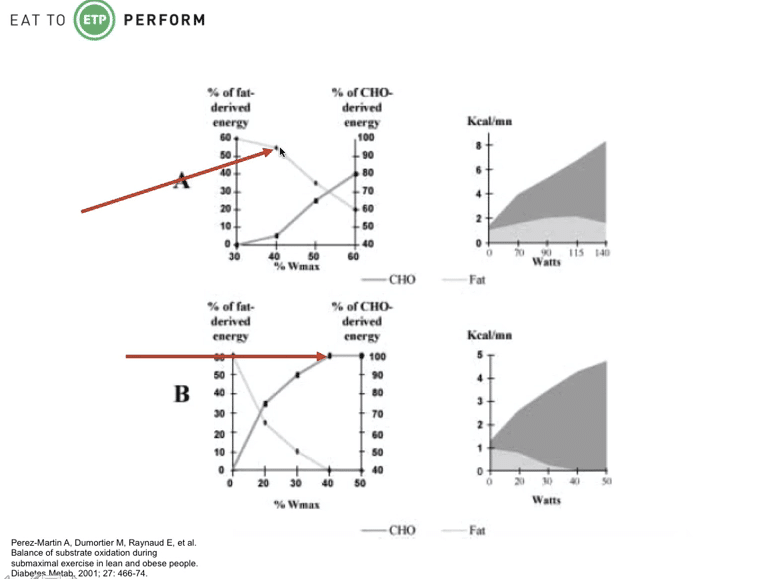
Not only is their baseline metabolism of fat impaired, their ability to utilize fat during exercise is also impaired. Individuals with T2DM rely more heavily on carbohydrates than fat at virtually all levels of exercise compared to their lean and healthy counterparts. In the figure below, look at the relative contributions of fat and carbohydrate toward energy production in a “lean” (top) and an “obese” (bottom) individual at identical, low level relative efforts. The lean person uses about 55% fat and 45% carbohydrate while the obese individual is almost exclusively carbohydrate metabolism. And it is not because there is not enough fat around, they have high levels of free fatty acids in the blood and intramuscular fat; they have a problem in turning that fat into usable energy.
Now there is another important piece of data I think we need to address as it points to a fairly big observation.
It has been clearly demonstrated that the issue with glucose metabolism in individuals with T2DM comes down to transporting glucose into cells, not the actual biochemical utilization of the glucose (3).
I think this is actually a fairly important observation in regards to applied nutrition and exercise for the following reasons:
(1) Glucose disposal (a fancy word for getting sugar into cells) can be increased in individuals with diabetes or “impaired metabolism’s” immediately through a very simple intervention; exercise. Engaging in exercise results in an acute increase in glucose disposal both independent of insulin action and therefore temporarily improves insulin resistance. Exercise also improves fat metabolism in those individuals with impaired fat metabolism. This is a critical point. People with impaired fat metabolism can increase their ability to oxidize fat much more rapidly when they exercise!
(2) Basal insulin resistance can be improved through weight loss. Weight loss can be achieved and sustained through a combination of diet and exercise.
(3) It suggests that carbohydrates themselves are actually not the major culprit.
The Wrap Up
The presented data points to the same conclusion: individuals who have T2DM, pre-diabetes, metabolic syndrome, or are somewhere along that spectrum most likely have a fat metabolism problem which likely leads to a glucose disposal problem. Exercise and weight loss work in conjunction with each other to improve both carbohydrate utilization and overall metabolism acutely.
References